
A half-micron structure most of us were never taught about may be the key to understanding why our patients leak. Time, not fluid, is the real treatment.
If you have spent any length of time practising acute medicine in Malaysia, the word "dengue" elicits something closer to weariness than alarm. We know the disease and its phases. We can recite the warning signs in our sleep. Indeed many of us have, on call. Every monsoon season brings another surge, another corridor of patients on charts of strict input-output, another round of haematocrit chasing.
And yet, for all our familiarity, there is a question most of us have stopped asking: why do dengue patients leak the way they do? The textbook answer is about "increased capillary permeability". A that phrase has always been a placeholder. Why, at the molecular level, does plasma rush out of the vasculature in a matter of hours, leaving the patient hypovolaemic despite a total body fluid excess?
The answer, it turns out, has been sitting in front of us for over a century. We just could not see it.
A Forgotten Equation
In 1896, Ernest Henry Starling who was a physiologist working at Guy's Hospital in London published a paper titled On the absorption of fluids from the connective tissue spaces. From it came the equation every medical student learns: fluid movement across a capillary wall is governed by the balance of hydrostatic and oncotic pressures, modulated by a permeability constant. Filtration at the arteriolar end. Absorption at the venular end. Roughly 90% reabsorbed venously. The remaining 10% returns through the lymphatics. Elegant, intuitive, and as we now know, is significantly incomplete.
The traditional Starling model describes a world in which the capillary wall is the only barrier worth modelling. But the capillary wall is not the only barrier. There is something else, something that the electron microscopists of the 1960s caught glimpses of but could not fully characterise, and that physiologists in the 1990s and 2000s finally brought into sharp focus.
It is called the endothelial glycocalyx. And it changes everything.
The Half-Micron Forest
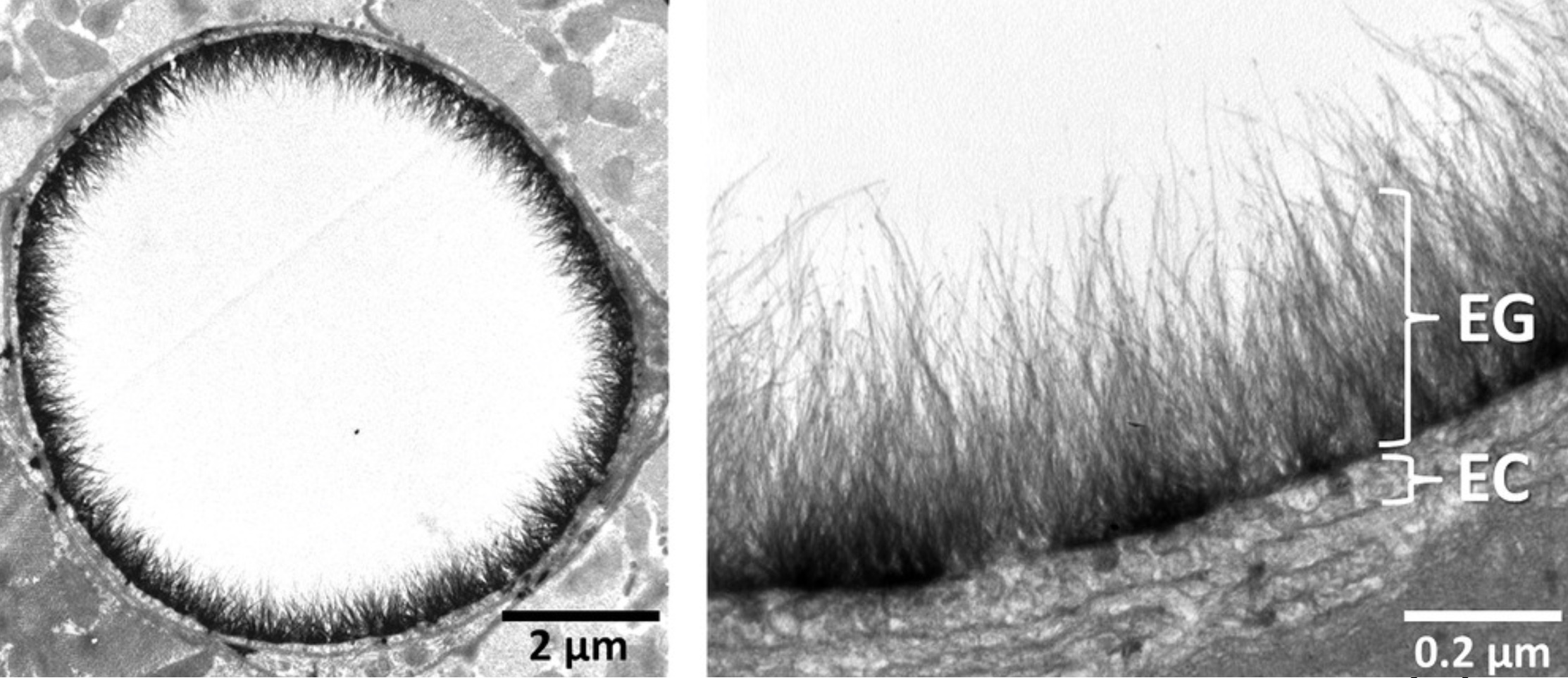
The glycocalyx is a mesh of proteoglycans, glycoproteins, and glycosaminoglycans that lines the luminal surface of every blood vessel in the human body. Half a micron to five microns thick. Negatively charged. It is a dynamic structure that is constantly shed and replenished. It is, in the most literal sense, a molecular forest projecting into the bloodstream from the endothelial surface.
What does it do? Almost everything that matters for vascular homeostasis. It maintains barrier function. It prevents leucocytes and platelets from adhering where they should not. It modulates the clotting cascade. It regulates nitric oxide-dependent vasodilation. And crucially for the revised Starling equation, it is the structure that determines the true oncotic gradient that holds plasma inside the vessel.
The revised Starling principle, formalised by Levick and Michel in 2010, replaces the interstitial oncotic pressure (πᵢ) with a sub-glycocalyx oncotic pressure (πg). The implications are profound. In steady state, there is no significant venous reabsorption. Filtered fluid returns to the circulation almost entirely via the lymphatics. The glycocalyx, not the endothelial cell membrane, is the molecular sieve that decides who stays in and who goes out.
If you have never been taught this, you are not alone. Most of us trained in an era when the glycocalyx was a footnote, if it appeared at all. But once you understand it, the pathophysiology of dengue stops being a mystery and becomes a story you can follow.
NS1: The Drill
Dengue virus produces a non-structural protein called NS1. It is secreted into the bloodstream during active infection. For years, NS1 was used primarily as a diagnostic marker, a useful early indicator of dengue infection, easily detected by lateral flow assay. But NS1 is not just a marker. It is a weapon.
Avirutnan and colleagues demonstrated in 2007 that secreted NS1 binds directly to heparan sulphate and chondroitin sulphate E on the surface of endothelial cells. Heparansulphate happens to make up more than 50% of the glycocalyx. The binding is not incidental. It is destructive. NS1 strips the glycocalyx of its primary structural component, and once that scaffold is gone, the barrier collapses.
The cytokine storm that accompanies severe dengue, TNF-α, IL-6, IL-8, complement activation generating C3a and C5a, compounds the damage. Direct endothelial infection adds another layer. By the time the patient presents with narrowing pulse pressure and rising haematocrit, the glycocalyx has been substantially degraded across the entire vascular tree.
Plasma leakage in dengue is not vague "capillary permeability." It is a specific molecular assault on a specific structure.
A Number That Should Trouble You
Glycocalyx destruction can be measured. When the structure breaks down, syndecan-1, a core proteoglycan, is shed into the bloodstream. Higher levels mean more damage. The numbers across different conditions tell a story that is, to put it mildly, instructive:
- Healthy controls: approximately 26 ng/mL
- Chronic kidney disease: 90 ng/mL
- Septic shock in the ICU: 246 ng/mL
- Severe dengue with severe plasma leakage: 2,614 ng/mL
Read that last number again. It is roughly 100 times the value seen in healthy controls and more than ten times the value seen in septic shock. Dengue does not merely damage the glycocalyx in the way other critical illnesses do. It obliterates it. Whatever mental model you hold for septic shock, and most of us have spent years building that model, dengue plasma leakage operates on a different scale entirely.
Why Diabetic Patients Do Worse
There is a second, related observation that should change how we risk-stratify our dengue patients. Type 2 diabetes is an independent risk factor for severe dengue, with an adjusted odds ratio of approximately 6.2. We have known this clinically for years. The glycocalyx tells us why.
Diabetic patients have baseline glycocalyx degradation. Sublingual imaging studies have shown that glycocalyx dimensions are significantly reduced in T2DM compared to controls, with red cells flowing closer to the vessel wall than they should. The forest is already thin. So when NS1 arrives and starts stripping heparan sulphate, there is almost nothing left to strip. The barrier collapses faster, the leakage is more severe, and the shock arrives earlier and harder.
This reframes a familiar clinical observation as a molecular inevitability. It is not a coincidence that our diabetic dengue patients deteriorate faster. They start the fight with half their armour already gone.
The Wills Trial, Reread
In 2005, Wills and colleagues published a landmark trial in the New England Journal of Medicine comparing three resuscitation fluids, Ringer's lactate, dextran 70, and starch, in 512 Vietnamese children with dengue shock syndrome. The trial is well known, but its deeper lesson is, in my experience, often missed.
In the early hours after resuscitation, colloids outperformed Ringer's lactate. Approximately 60% of patients receiving colloid achieved initial cardiovascular stability within the first hour, compared to about 50% with crystalloid. The difference was statistically significant (p = 0.02). Colloids appeared to win the sprint.
But here is the part that matters: by 48 hours, all three fluids had converged. The p-value at that point was 0.18 i.e. no significant difference between groups.
What had happened? The glycocalyx had begun to regenerate. As NS1 levels fell and the immune response cleared the virus, the molecular barrier that NS1 had stripped started to rebuild itself. The Starling equilibrium re-established. And once it did, it stopped mattering what had been hanging in the drip stand.
Colloids are not magic. They simply have molecules large enough that they leak through a damaged glycocalyx more slowly than crystalloids do. They buy time. And in dengue, time is not a delay before the treatment arrives — time is the treatment.
Our role as acute physicians is to keep the patient alive long enough for the biological clock to run out. That is the entire game.
Watching the Glycocalyx Scream
Even without sublingual microscopy, the glycocalyx tells us when it is failing. It tells us through the gallbladder.
A meta-analysis of ultrasound-detected gallbladder wall thickening (GBWT) in dengue showed a sensitivity of 0.88 (95% CI 0.77–0.94) and a specificity of 0.63 (95% CI 0.48–0.76) for predicting severe dengue. The pooled odds ratio for the association between increased GBWT and severe dengue was 2.35 (95% CI 1.88–2.82, p < 0.001).
Why the gallbladder, of all structures? Because the gallbladder wall is essentially a thin serous membrane and is exquisitely sensitive to plasma extravasation. When the systemic glycocalyx fails, fluid accumulates in serous spaces and tissue planes throughout the body. The gallbladder wall happens to be the easiest of those to image.
So when your medical officer rings you at 2 AM and tells you the gallbladder wall measures 8 millimetres on bedside ultrasound, do not dismiss it as incidental. That is not a surgical problem. That is a window into a systemic endothelial catastrophe. That is the glycocalyx screaming.
The Paradox at the Bedside
This brings us to the clinical paradox that confuses every houseman who encounters their first dengue shock patient. The patient is in hypovolaemic shock, manifesting narrow pulse pressure, tachycardia, cold peripheries, oliguria, despite total body fluid excess. They are dry inside the vessels and wet outside them. At the same time.
This is not what we learned about shock in medical school. Shock, we were taught, comes from inadequate intravascular volume. The treatment is to give volume. And in dengue, that is partially correct. We do need to restore intravascular volume. But the unique cruelty of dengue is that the fluid we administer follows the same path as the patient's own plasma: out of the vessels and into the third space.
This is why dengue fluid management is so unforgiving. We are running fluid into a system whose barrier has been molecularly dismantled. Too little fluid and the patient decompensates. Too much fluid and we drown the lungs and the abdomen.
A Framework for Management
The principles flow directly from the physiology:
1. Recognise the paradox
Hypovolaemic shock with total body fluid excess. Treat what you cannot see (intravascular depletion) without exacerbating what you can see (third-space accumulation).
2. Resuscitate aggressively in the early phase
Bridge the leakage. Colloids buy more time than crystalloids in the first critical hours, but the effect is temporary.
3. Monitor relentlessly
Haematocrit, pulse pressure, urine output. These are the surrogate markers of glycocalyx integrity that we have. Use them.
4. Stop fluids during recovery
This is the part we get wrong most often. When the glycocalyx regenerates, typically within 24 to 48 hours of defervescence, third-space fluid begins to return to the intravascular compartment. If you are still pushing fluids at that point, you will drown your patient from the inside. The transition from leakage to recovery is the most dangerous moment in dengue management, precisely because the treatment that saved the patient yesterday will harm them today.
The goal, simply stated: restore intravascular volume without worsening third-space loss. And know when to stop.
What This Means for Us
I have presented this material to senior clinicians around the country, and the question I am most often asked is: what do we actually do differently on Monday morning? The honest answer is: not much, in terms of protocol. Our existing dengue management guidelines, refined over decades of Malaysian clinical experience, remain sound. The CPG works. The fluid algorithms work.
What changes is the understanding we bring to the bedside. When we know that dengue plasma leakage is glycocalyx destruction at scale, we approach our diabetic dengue patients with appropriate gravity. We respect the gallbladder wall measurement. We resist the temptation to push more fluid when the patient stops responding. We recognise that the recovery phase is not a period of relaxation but the most dangerous transition in the disease course. And we accept, perhaps for the first time, that our role is not to fix the leak, because we cannot, but to buy the time the body needs to fix itself.
Acute medicine, properly understood, is rarely about adding something. It is about understanding what is already there. A half-micron structure that most of us were never taught about. Doing work that most of us never appreciated. Failing in ways that explain the disease we see every monsoon season.
The next time you stand at the bedside of a dengue patient, adjusting the fluid rate, watching the haematocrit, checking the pulse pressure, think about the glycocalyx. Think about NS1, drilling holes. Think about your role: not as someone who fixes the leakage, but as someone who buys time for the body to do what it knows how to do.
That is what acute medicine is.
Selected References
Avirutnan P, Zhang L, Punyadee N, et al. Secreted NS1 of dengue virus attaches to the surface of cells via interactions with heparan sulfate and chondroitin sulfate E. PLoS Pathogens. 2007;3(11):e183.
Broekhuizen LN, Lemkes BA, Mooij HL, et al. Effect of sulodexide on endothelial glycocalyx and vascular permeability in patients with type 2 diabetes mellitus. Diabetologia. 2010;53(12):2646–2655.
Chappell D, Jacob M, Hofmann-Kiefer K, et al. Hydrocortisone preserves the vascular barrier by protecting the endothelial glycocalyx. Anesthesiology. 2007;107(5):776–784.
Lam PK, McBride A, Le DHT, et al. Visual and biochemical evidence of glycocalyx disruption in human dengue infection, and association with plasma leakage severity. Frontiers in Medicine. 2020;7:545813.
Lee K, Hsieh CJ, Lee CT, Liu JW. Diabetic patients suffering dengue are at risk for development of dengue shock syndrome/severe dengue. Journal of Microbiology, Immunology and Infection. 2020;53(1):69–78.
Levick JR, Michel CC. Microvascular fluid exchange and the revised Starling principle. Cardiovascular Research. 2010;87(2):198–210.
Reitsma S, Slaaf DW, Vink H, et al. The endothelial glycocalyx: composition, functions, and visualisation. Pflugers Archiv. 2007;454(3):345–359.
Starling EH. On the absorption of fluids from the connective tissue spaces. Journal of Physiology. 1896;19(4):312–326.
Wills BA, Dung NM, Loan HT, et al. Comparison of three fluid solutions for resuscitation in dengue shock syndrome. New England Journal of Medicine. 2005;353(9):877–889.