
Introduction
The World Health Organization comprehensively defines health not merely as the absence of disease, but as a state of complete physical, psychological, social, and spiritual well-being.(1) However, in the high-stakes, fast-paced environment of acute medical care, the clinical focus frequently narrows exclusively to the biological. We treat the physical body and its disease processes, but in doing so, we risk neglecting the profound unity of the human soul. Caring for the spirit is, fundamentally, caring for the whole person. Spirituality is a universal human experience, a continuous search for meaning, purpose, and connection that can exist entirely independently of organized religion.(2) This article explores the vital integration of spiritual support in acute care, illustrating through five diverse clinical cases how physicians can address the biological, psychological, social, and spiritual dimensions of their patients to promote true healing.
The Spectrum of Spiritual Needs in Acute Illness
When a patient is admitted to an acute care ward, they bring more than just a failing organ or an infectious disease; they carry a profound narrative and a vulnerable spirit. Acute illness routinely strips individuals of their autonomy and confronts them with intense spiritual needs. These needs often manifest as an acute fear of death and suffering, a crippling loss of control and helplessness, feelings of guilt or regret, a deep desire for connection with family or a faith community, and overwhelming existential questions regarding God, fate, and life's meaning.
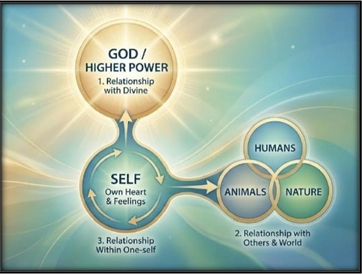
When these profound needs are unmet, patients fall into spiritual distress; a state of suffering caused by an impaired ability to experience meaning in life through connections with the self, others, the world, or a higher power [Figure 1]. Patients in distress may feel angry at God about a diagnosis, struggle to find meaning in their suffering, or experience emotional pain and isolation that severely impacts their daily functioning.(2,3) This distress does not operate in a vacuum; it creates a vicious cycle where spiritual anguish exacerbates physical symptoms like pain and fatigue, which in turn heighten emotional symptoms like anxiety and sadness.
If left unaddressed, distress can escalate into a spiritual crisis. A spiritual crisis is an acute, severe state that completely exceeds a person's resources to cope, leading to significant suffering and a potential psychological or existential breakdown. (3.4) A patient in crisis might express a profound loss of the will to live, believe they are unforgivable or damned, or completely reject their previously held beliefs in a state of turmoil, requiring urgent assessment and collaborative intervention with mental health professionals.
The Physician’s Role: Presence is Medicine
As physicians, our primary training and instinct is to diagnose and "fix." Yet, when a patient asks, "Why is this happening to me?" or cries out, "Please don't let me die, I'm not ready yet," offering an empty reassurance like "Don't worry, you'll be fine" dismisses their profound fear. Instead, a spiritually attuned physician leans into the discomfort. A helpful, healing response validates the emotion and invites exploration: "It sounds like you're very afraid... what is it that makes you feel not ready?". Compassion is not just an emotion; it is a healing presence that transforms a routine clinical encounter into a sacred moment. Even 30 seconds of intentional, undivided presence can be immensely healing in an acute care setting. Physicians can seamlessly integrate this into daily rounds using practical frameworks like the Ask-Affirm-Act model:(3,4)
- Ask: "What gives you strength during difficult times?"
- Affirm: "That sounds important to you."
- Act: Offer appropriate faith or community support.
For a deeper evaluation, the FICA Model guides clinicians to assess a patient's Faith and belief, the Importance and influence of those beliefs, their Community connections, and how they wish these to be Addressed in their medical care.(4,5) Ultimately, the most actionable steps any physician can take are simple yet profound: Pause and Listen (even briefly), Acknowledge and Empathize (reflecting feelings, not just facts), and Connect and Refer to chaplains, counselors, or family support.
Alongside tools like FICA and Ask-Affirm-Act, the HOPE model serves as another highly effective, structured framework for clinical evaluation. Originally designed to teach medical learners how to conduct a spiritual assessment, the mnemonic guides clinicians to systematically ask about sources of Hope (meaning, comfort, and strength), Organized religion, Personal spirituality and practices, and the Effects of these beliefs on medical care and end-oflife decisions. A major clinical advantage of the HOPE tool is its gradual approach: its initial questions intentionally avoid potentially polarizing words like "faith" or "religion," instead gently asking patients about their sources of comfort and peace to minimize communication barriers. This non-threatening entry point is especially crucial in acute, high-stress settings where building rapid rapport is essential.
Case Studies: Translating Theory to Holistic Practice
The biopsychosocial-spiritual model comes to life when applied to real clinical scenarios. The following five cases demonstrate the complex interplay of these four domains and the absolute necessity of holistic management.
Case 1: The Young Gentleman with COVID-19
A young adult male developed heart failure secondary to post-COVID myocarditis. Biologically, he suffered from fatigue, breathlessness, and reduced exercise tolerance that required medications and major lifestyle adjustments. Psychologically, he was deeply anxious about his prognosis, frustrated by his new physical limits, and depressed by his loss of independence and uncertainty about the future. Socially, his family faced financial and care giving strain while he struggled to return to work, feeling isolated from peers who did not understand his condition.
Crucially, his spiritual struggle was defined by a profound loss of hope and the agonizing question, "Why me at this age?”. Holistic management for this patient requires much more than heart failure medications. It necessitates psychological support for his anxiety, social work intervention for his family's financial strain, and spiritual care to help him find meaning and hope, potentially drawing strength from prayer, faith, or reframing his illness as a test of resilience.
Case 2: The Young Lady with Pseudo-Stroke
A 42-year-old woman with Type 2 Diabetes presented with sudden weakness initially mimicking a stroke. Neuroimaging was normal, leading to a diagnosis of Functional Neurological Disorder (FND) triggered by immense psychosocial stress. Her psychological distress stemmed from acute marital conflict, impending divorce, and grief from a previous widowhood, compounded by this second marital breakdown. Socially, she navigated complex blended family dynamics, stepchild jealousy, and active legal stress, with divorce proceedings initiated at the Syariah court just before her symptom onset. Spiritually, the patient noted that her illness onset occurred immediately after prayer, which intensified her spiritual questioning. She struggled with feelings of unfairness and questioned whether her illness was a divine trial or a punishment. Her holistic management plan had to integrate medical care for her diabetes with psychological therapy for stress and coping, social support for her family dynamics, and, vitally, spiritual care to restore her sense of hope and meaning.
Case 3: The Boy with Cat-Scratch Marks
A young man with Type 1 Diabetes suffered from recurrent Diabetic Ketoacidosis (DKA), malnutrition due to food insecurity, and physical fatigue, alongside a high infection risk exacerbated by unsafe cat scratches and poor wound care. Psychologically, he exhibited maladaptive coping mechanisms, low self-esteem, loneliness after his brother moved away, and severe feelings of hopelessness and worthlessness. Socially, his family struggled financially, and he faced isolation from his peers. His spiritual assessment revealed profound spiritual distress with the potential for a full spiritual crisis. He felt a complete loss of purpose, questioned his role in society, and perceived his illness as a punishment or curse. Interestingly, his only anchor for connection and comfort was caring for his pet cat. Urgent intervention was needed. Alongside wound care and diabetes management, his care plan required exploring his relationship with his cat as a source of connection and hope, aiming to reframe his illness as a challenge that could open new avenues for meaningful contribution.
Case 4: The 6th Child
In the neonatal intensive care unit (NICU), Baby M, born with Noonan's Syndrome, faced a poor prognosis due to pneumonia and recurrent hospitalizations. A non-intubation decision was made, transitioning the infant toward end-of-life care. His mother, experienced intense psychological strain: anticipatory grief, fear of her child's death, and profound caregiver burnout. Socially, the family's life was entirely reorganized; they closed their business, moved homes, and faced significant financial constraints and extended family tension, though the husband provided strong support. Spiritually, the mother exhibited deep faith, relying heavily on God’s will and daily prayers for either healing or a peaceful passing. However, she also suffered ongoing spiritual distress and guilt linked to an initial intention to abort the pregnancy, leading her to interpret her child's illness as a divine punishment. Her care required faith-based spiritual guidance and meaningmaking, addressing her spiritual guilt alongside end-of-life medical support for Baby M, and grief counseling for the family.
Case 5: The Fatal Fake Braces
A 24-year-old mother of three, developed severe sepsis from infective endocarditis linked to fake dental braces. Her prolonged stay in the Critical Care Unit occurred just one month postpartum after delivering a premature baby at 27 weeks. Biologically restricted and facing a long 6-8 week recovery, her psychological state deteriorated into tearfulness, helplessness, and a high risk for postpartum depression, exacerbated by prolonged separation from her newborn. Socially, her husband was the sole breadwinner on a limited security guard income, making transport to her newborn's distant hospital impossible. Spiritually, she felt a devastating loss of meaning and purpose tied to her maternal identity. She felt deeply disconnected from her children and in despair regarding her inability to fulfill her role as a mother. Her spiritual care opportunities focused on reassurance and meaning-making. Clinicians needed to facilitate virtual connections with her baby (via photos and video calls), encourage her to reframe motherhood beyond mere physical presence, and involve a chaplain or pastoral care provider for spiritual strengthening to affirm her maternal value despite her severe illness.
Conclusion
The integration of spiritual care in the acute setting is not a peripheral luxury; it is a clinical imperative. As beautifully noted in Islamic tradition, "Be merciful to those on earth, and the Most Merciful will show mercy to you," reminding us that compassion is a core tenet of healing.(6) Every patient we encounter carries a unique story and a resilient, yet vulnerable, spirit. Addressing their spirituality is fundamentally an act of addressing their humanity.(7) While the marvels of modern science allow us to heal the physical body, it is our human compassion that heals the soul. By committing to holistic care; balancing the biological, psychological, social, and spiritual, we embody the ultimate truth of our profession.(8) "Presence is medicine: We may not cure, but we can care".
References
1. World Health Organization. The Geneva Charter for well-being. Geneva: World Health Organization; 2021. Accessed May 31, 2026. https://www.who.int/publications/m/item/the-geneva-charter-for-well-being
2. Abuatiq A. Spiritual Care for Critical Care Patients. Int J Nurs Clin Pract. 2015;2:128.
3. Kuckel DP, Jones AL, Smith DK. The Spiritual Assessment. Am Fam Physician. 2022;106(4):415-419.
4. Puchalski C, Romer AL. Taking a spiritual history allows clinicians to understand patients more fully. J Palliat Med. 2000;3(1):129-137.
5. Puchalski CM. The FICA spiritual history tool. J Palliat Med. 2014;17(1):105-106.
6. Swihart DL, Yarrarapu SNS, Martin RL. Cultural Religious Competence in Clinical Practice. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026.
7. Rustam JS, Fahdya N. Spiritual well-being among critically ill patients: A literature review. Medika Aksara: Jurnal of Health Sciences. 2025;1(1):92- 98.
8. Sulmasy DP. A biopsychosocial-spiritual model for the care of patients at the end of life. Gerontologist. 2002;42(spec no 3):24-33.